Drug combinations: Difference between revisions
No edit summary |
GrimReaper (talk | contribs) No edit summary |
||
| Line 1: | Line 1: | ||
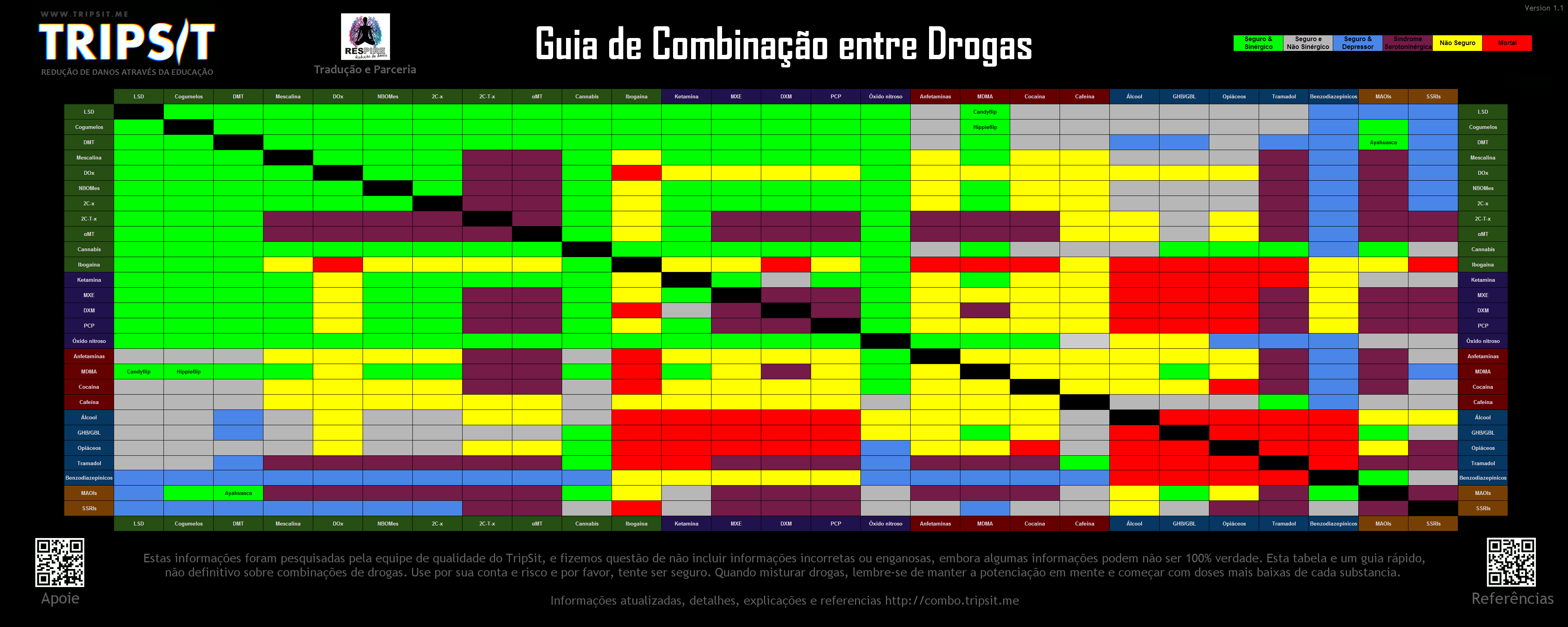
'''WARNING! For educational purposes: We do not endorse any of these combinations. This page will always be 'work in progress'. It is extremely important to be safe at all times! ''' | '''WARNING! For educational purposes: We do not endorse any of these combinations. This page will always be 'work in progress'. It is extremely important to be safe at all times! ''' | ||
[[File: | [[File:TripSitDrugComboChart.gif|1000px|center]] | ||
== Overview == | == Overview == | ||
Revision as of 12:57, 14 October 2015
WARNING! For educational purposes: We do not endorse any of these combinations. This page will always be 'work in progress'. It is extremely important to be safe at all times!
{kind=link}
Overview
If you want to give us some feedback/recommendation/comment on the chart, you can contact us:
Email: [email protected], or email GrimReaper directly at [email protected]
Chart versions
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Specific Combinations
Amphetamine & Mescaline
The focus and anxiety caused by stimulants is magnified by psychedelics and results in an increased risk of thought loops
Cocaine & Mescaline
The focus and anxiety caused by stimulants is magnified by psychedelics and results in an increased risk of thought loops
Caffeine & Mescaline
High doses of caffeine are uncomfortable and this will be magnified by psychedelics
5-meo-xxt & Mescaline
The 5-MeO class of tryptamines can be unpredictable in their interactions
Tramadol & Mescaline
This combination can cause seizures due to the lowering of the threshold by tramadol and the potential of mescaline to cause seziures.
5-meo-xxt & Dox
The 5-MeO class of tryptamines can be unpredictable in their interactions, particularly increasing the risk of unpleasant physical side effects.
Ketamine & Dox
Ketamine and psychedelics tend to potentiate each other - go slowly.
MXE & Dox
As an NMDA antagonist MXE potentiates DOx which can be unpleasantly intense
DXM & Dox
The DOx class as psychedelic stimulants have the potential to mask the effects of DXM and could lead to redosing to an unsafe level. DXM can also potentiate DOx resulting in an unpleasantly intense experience.
PCP & Dox
Details of this combination are not well understood but PCP generally interacts in an unpredictable manner.
Amphetamine & Dox
The combined stimulating effects of the two can lead to an uncomfortable body-load, while the focusing effects of amphetamine can easily lead to thought loops. Coming down from amphetamines while the DOx is still active can be quite anxiogenic.
MDMA & Dox
The combined stimulating effects of the two can be uncomfortable. Coming down on the MDMA while the DOx is still active can be quite anxiogenic.
Cocaine & Dox
The combined stimulating effects of the two can lead to an uncomfortable body-load, while the focusing effects of cocaine can easily lead to thought loops. Coming down from cocaine while the DOx is still active can be quite anxiogenic
Caffeine & Dox
High doses of caffeine may cause anxiety which is less manageable when tripping, and since both are stimulating it may cause some physical discomfort.
Alcohol & Dox
Drinking on stimulants is risky because the sedative effects of the alcohol are reduced, and these are what the body uses to gauge drunkenness. This typically leads to excessive drinking with greatly reduced inhibitions, high risk of liver damage and increased dehydration. They will also allow you to drink past a point where you might normally pass out, increasing the risk.
Opioids & Dox
No unexpected interactions.
Tramadol & Dox
Tramadol is well known to lower seizure threshold and psychedelics also cause occasional seizures.
5-meo-xxt & Nbomes
The 5-MeO class of tryptamines can be unpredictable in their interactions and the NBOMes are known to be unpredictable even alone. This combination is best avoided
Amphetamine & Nbomes
Amphetamines and NBOMes both provide considerable stimulation. When combined they can result in tachycardia, hypertension, vasoconstriction and in extreme cases heart failure. The anxiogenic and focusing effects of stimulants are also not good in combination with psychedelics as they can lead to unpleasant thought loops. NBOMes are known to cause seizures and stimulants can increase this risk.
Cocaine & Nbomes
Cocaine and NBOMes both provide considerable stimulation. When combined they can result in severe vasoconstriction, tachycardia, hypertension, and in extreme cases heart failure.
Caffeine & Nbomes
Caffiene can bring out the natural stimulation from psychedelic drugs to make it uncomfortable. High doses can cause anxiety which is hard to handle while tripping
Tramadol & Nbomes
Tramadol is well known to lower seizure threshold and NBOMes have also shown a tendency to cause severe seizures
5-meo-xxt & 2c-x
The 5-MeO psychedelics can interact unpredictably to potentiate other psychedelics
Amphetamine & 2c-x
The anxiogenic and focusing effects of stimulants increase the chance of unpleasant thought loops. The combination is generally uneccessary because of the stimulating effects of psychedelics. Combination of the stimulating effects may be uncomfortable.
Cocaine & 2c-x
The anxiogenic and focusing effects of stimulants increase the chance of unpleasant thought loops. The combination is generally unnecessary because of the stimulating effects of psychedelics. Combination of the stimulating effects may be uncomfortable.
Caffeine & 2c-x
High doses of caffeine may cause anxiety which is less manageable when tripping, and since both are stimulating the combination may cause some physical discomfort.
Tramadol & 2c-x
Tramadol is well known to lower seizure threshold and psychedelics raise the risk of seizures.
Caffeine & 2c-t-x
High doses of caffeine may cause anxiety which is less manageable when tripping, and since both are stimulating the combination may cause some physical discomfort.
Alcohol & 2c-t-x
Both these classes of compound can interact unpredictably. Caution should be exercised.
Opioids & 2c-t-x
No expected interactions, some Opioids have Serotonin action, and could lead to Serotonin Syndrome or a seizure. These are pretty much only to Pentazocine, Methadone, Tramadol, Tapenatdol.
Caffeine & αMT
High doses of caffeine may cause anxiety which is less manageable when tripping, and since both are stimulating the combination may cause some physical discomfort.
Alcohol & αMT
aMT has a broad mechanism of action in the brain and so does alcohol so the combination can be unpredictable
Opioids & αMT
No unexpected interactions
Amphetamine & 5-meo-xxt
The anxiogenic and focusing effects of stimulants increase the chance of unpleasant thought loops. The combination is generally unnecessary because of the stimulating effects of psychedelics.
MDMA & 5-meo-xxt
Some of the 5-MeO tryptamines are a bit unpredictable and should be mixed with MDMA with care
Cocaine & 5-meo-xxt
The anxiogenic and focusing effects of stimulants increase the chance of unpleasant thought loops. The combination is generally unnecessary because of the stimulating effects of psychedelics.
Amphetamine & Ketamine
No unexpected interactions. Likely to increase blood pressure but not an issue with sensible doses
Caffeine & Ketamine
No unexpected interactions.
Alcohol & Ketamine
Both substances cause ataxia and bring a very high risk of vomiting and unconsciousness. If the user falls unconscious while under the influence there is a severe risk of vomit aspiration if they are not placed in the recovery position.
Ghb/gbl & Ketamine
Both substances cause ataxia and bring a risk of vomiting and unconsciousness. If the user falls unconscious while under the influence there is a severe risk of vomit aspiration if they are not placed in the recovery position.
Opioids & Ketamine
Both substances bring a risk of vomiting and unconsciousness. If the user falls unconscious while under the influence there is a severe risk of vomit aspiration if they are not placed in the recovery position.
Tramadol & Ketamine
No unexpected interactions
Benzodiazepines & Ketamine
Both substances potentiate the ataxia and sedation caused by the other and can lead to unexpected loss of consciousness at high doses. While unconscious, vomit aspiration is a risk if not placed in the recovery position.
Amphetamine & MXE
Risk of tachycardia, hypertension, and manic states
MDMA & MXE
There have been reports of risky serotonergic interactions when the two are taken at the same time, but MXE taken to the end of an MDMA experience does not appear to cause the same issues.
Cocaine & MXE
Stimulants taken with MXE can lead to hypermanic states much more easily, especially if sleep is avoided.
Caffeine & MXE
No likely interactions
Alcohol & MXE
There is a high risk of memory loss, vomiting and severe ataxia from this combination.
Ghb/gbl & MXE
Both substances cause ataxia and bring a risk of vomiting and unconsciousness. If the patient falls unconscious while under the influence there is a severe risk of vomit aspiration if they are not placed in the recovery position.
Opioids & MXE
This combination can potentiate the effects of the opioid
Benzodiazepines & MXE
Both substances potentiate the ataxia and sedation caused by the other and can lead to unexpected loss of consciousness at high doses. Place affected patients in the recovery position to prevent vomit aspiration from excess.
Ssris & MXE
Depending on the SSRI this combination can be unpredictable
Amphetamine & DXM
Both substances raise heart rate, in extreme cases, panic attacks caused by these drugs have led to more serious heart issues.
Maois & DXM
High risk of serotonin syndrome
Cocaine & DXM
Both substances raise heart rate, in extreme cases, panic attacks caused by these drugs have led to more serious heart issues
Ssris & DXM
High risk of serotonin syndrome.
Caffeine & DXM
High doses of caffeine may cause anxiety which is less manageable when tripping, and since both are stimulating the combination may cause some physical discomfort.
Alcohol & DXM
Both substances potentiate the ataxia and sedation caused by the other and can lead to unexpected loss of consciousness at high doses. Place affected patients in the recovery position to prevent vomit aspiration from excess. Additionally CNS depression can lead to difficulty breathing. Avoid on anything higher than 1st plateau.
Ghb/gbl & DXM
Both substances cause ataxia and bring a risk of vomiting and unconsciousness. If the patient falls unconscious while under the influence there is a severe risk of vomit aspiration if they are not placed in the recovery position. This combination is hard to predict
Opioids & DXM
CNS depression, difficult breathing, heart issues, hepatoxic, just very unsafe combination all around. Additionally, there is a reverse cross tolerance between opiates/dxm. I.E. if one takes dxm, their tolerance of opiates goes down slightly, thus causing additional synergistic effects.
Benzodiazepines & DXM
Small doses of benzos can end a bad trip, but both substances potentiate the ataxia and sedation caused by the other and this can lead to unexpected loss of consciousness at high doses. While unconscious, vomit aspiration is a risk if not placed in the recovery position.
Amphetamine & PCP
This combination can easily lead to hypermanic states
MDMA & PCP
This combination can easily lead to hypermanic states
Cocaine & PCP
This combination can easily lead to hypermanic states
Caffeine & PCP
Details of this combination are not well understood but PCP generally interacts in an unpredictable manner.
Alcohol & PCP
Details of this combination are not well understood but PCP generally interacts in an unpredictable manner.
Ghb/gbl & PCP
Details of this combination are not well understood but PCP generally interacts in an unpredictable manner.
Opioids & PCP
PCP can reduce opioid tolerance, increasing the risk of overdose
Benzodiazepines & PCP
Both substances potentiate the ataxia and sedation caused by the other and can lead to unexpected loss of consciousness at high doses. While unconscious, vomit aspiration is a risk if not placed in the recovery position. Memory blackouts are likely
Ssris & PCP
Details of this combination are not well understood but PCP generally interacts in an unpredictable manner.
Alcohol & N2O
This combination can lead to vomiting
Ghb/gbl & N2O
MDMA & Amphetamine
Amphetamines increase the neurotoxic effects of MDMA
Cocaine & Amphetamine
This combination of stimulants will increase strain on the heart. It is not generally worth it as cocaine has a mild blocking effect on dopamine releasers like amphetamine
Caffeine & Amphetamine
This combination of stimulants is not generally necessary and may increase strain on the heart, as well as potentially causing anxiety and greater physical discomfort.
Alcohol & Amphetamine
Drinking on stimulants is risky because the sedative effects of the alcohol are reduced, and these are what the body uses to gauge drunkenness. This typically leads to excessive drinking with greatly reduced inhibitions, high risk of liver damage and increased dehydration. They will also allow you to drink past a point where you might normally pass out, increasing the risk. If you do decide to do this then you should set a limit of how much you will drink each hour and stick to it, bearing in mind that you will feel the alcohol and the stimulant less. Extended release formulations may severely impede sleep, further worsening the hangover.
Ghb/gbl & Amphetamine
Stimulants increase respiration rate allowing a higher dose of sedatives. If the stimulant wears off first then the opiate may overcome the patient and cause respiratory arrest.
Opioids & Amphetamine
Stimulants increase respiration rate allowing a higher dose of opiates. If the stimulant wears off first then the opiate may overcome the patient and cause respiratory arrest.
Tramadol & Amphetamine
Tramadol and stimulants both increase the risk of seizures.
Cocaine & MDMA
Cocaine blocks some of the desirable effects of MDMA while increasing the risk of heart attack.
Caffeine & MDMA
Caffiene is not really necessary with MDMA and increases any neurotoxic effects from MDMA
Alcohol & MDMA
Both MDMA and alcohol cause severe dehydration. Approach this combination with caution, moderation and sufficient hydration.
Tramadol & MDMA
Tramadol and stimulants both increase the risk of seizures.
Caffeine & Cocaine
Both stimulants, risk of tachycardia, hypertension, and in extreme cases heart failure.
Alcohol & Cocaine
Drinking on stimulants is risky because the sedative effects of the alcohol are reduced, and these are what the body uses to gauge drunkenness. This typically leads to excessive drinking with greatly reduced inhibitions, high risk of liver damage and increased dehydration. They will also allow you to drink past a point where you might normally pass out, increasing the risk. If you do decide to do this then you should set a limit of how much you will drink each hour and stick to it, bearing in mind that you will feel he alcohol less. Cocaine is potentiated somewhat by alcohol because of the formation of cocaethylene.
Ghb/gbl & Cocaine
Stimulants increase respiration rate allowing a higher dose of sedatives. If the stimulant wears off first then the opiate may overcome the patient and cause respiratory arrest. Likewise the G can wear off and leave a dangerous concentration of cocaine behind
Opioids & Cocaine
Stimulants increase respiration rate allowing a higher dose of opiates. If the stimulant wears off first then the opiate may overcome the patient and cause respiratory arrest.
Tramadol & Cocaine
Tramadol and stimulants both increase the risk of seizures.
Ssris & Cocaine
Risk of serotonin syndrome, Likely to make the SSRI's innefective with regular cocaine use. The SSRIs may also make the cocaine less effective. Mental stability and cocaine don't go together
Ghb/gbl & Alcohol
Even in very low doses this combination rapidly leads to memory loss, severe ataxia and unconsciousness. There is a high risk of vomit aspiration while unconscious.
Opioids & Alcohol
Both substances potentiate the ataxia and sedation caused by the other and can lead to unexpected loss of consciousness at high doses. Place affected patients in the recovery position to prevent vomit aspiration from excess. Memory blackouts are likely
Tramadol & Alcohol
Heavy CNS depressants, risk of seizures. Both substances potentiate the ataxia and sedation caused by the other and can lead to unexpected loss of consciousness at high doses. Place affected patients in the recovery position to prevent vomit aspiration from excess. Memory blackouts are likely.
Benzodiazepines & Alcohol
Ethanol ingestion may potentiate the CNS effects of many benzodiazepines. The two substances potentiate each other strongly and unpredictably, very rapidly leading to unconsciousness. While unconscious, vomit aspiration is a risk if not placed in the recovery position. Blacking out and memory loss is almost certain.
MAOIs & Alcohol
The chemical tyramine in alcoholic beverages can have dangerous reactions with MAOIs, causing an increase in blood pressure.
Ssris & Alcohol
Alcohol may potentiate some of the pharmacologic effects of CNS-active agents. Use in combination may result in additive central nervous system depression and/or impairment of judgment, thinking, and psychomotor skills.
Opioids & Ghb/gbl
The two substances potentiate each other strongly and unpredictably, very rapidly leading to unconsciousness. While unconscious, vomit aspiration is a risk if not placed in the recovery position
Tramadol & Ghb/gbl
The sedative effects of this combination can lead to dangerous respiratory depression.
Benzodiazepines & Ghb/gbl
The two substances potentiate each other strongly and unpredictably, very rapidly leading to unconsciousness. While unconscious, vomit aspiration is a risk if not placed in the recovery position.
Tramadol & Opioids
Concomitant use of tramadol increases the seizure risk in patients taking other opioids. These agents are often individually epileptogenic and may have additive effects on seizure threshold during coadministration. Central nervous system- and/or respiratory-depressant effects may be additively or synergistically present
Benzodiazepines & Opioids
Central nervous system and/or respiratory-depressant effects may be additively or synergistically present. The two substances potentiate each other strongly and unpredictably, very rapidly leading to unconsciousness. While unconscious, vomit aspiration is a risk if not placed in the recovery position Blackouts/memory loss likely
Maois & Opioids
Coadministration of monoamine oxidase inhibitors (MAOIs) with certain opioids has been associated with rare reports of severe and fatal adverse reactions. There appear to be two types of interaction, an excitatory and a depressive one. Symptoms of the excitatory reaction may include agitation, headache, diaphoresis, hyperpyrexia, flushing, shivering, myoclonus, rigidity, tremor, diarrhea, hypertension, tachycardia, seizures, and coma. Death has occurred in some cases.
Benzodiazepines & Tramadol
Central nervous system- and/or respiratory-depressant effects may be additively or synergistically present. Vomit aspiration a risk when passed out, lay down in recovery position if ingested.
References
LSD & DMT
http://www.ncbi.nlm.nih.gov/pubmed/3006089 http://deepblue.lib.umich.edu/bitstream/handle/2027.42/26285/0000370.pdf
LSD & GHB/GBL
http://www.ncbi.nlm.nih.gov/pubmed/16483730
LSD & Opioids
http://www.ncbi.nlm.nih.gov/pubmed/547279
http://www.ncbi.nlm.nih.gov/pubmed/3006089
"Low doses antagonized the effects of both hallucinogens, whereas larger doses enhanced their effects."
http://www.ncbi.nlm.nih.gov/pubmed/3006089
http://deepblue.lib.umich.edu/bitstream/handle/2027.42/26285/0000370.pdf
LSD & Tramadol
http://www.ncbi.nlm.nih.gov/pubmed/3006089
LSD & MAOIs
http://www.ncbi.nlm.nih.gov/pubmed/8788508
http://www.ncbi.nlm.nih.gov/pubmed/108709
https://www.erowid.org/references/refs_view.php?A=ShowDocPartFrame&ID=2439&DocPartID=2199
LSD & SSRIs
http://www.nature.com/npp/journal/v14/n6/full/1380431a.html
http://www.ncbi.nlm.nih.gov/pubmed/8726753
DMT & Opioids
http://www.ncbi.nlm.nih.gov/pubmed/3006089
DMT & Tramadol
http://www.ncbi.nlm.nih.gov/pubmed/3006089
MDMA & GHB/GBL
http://www.ncbi.nlm.nih.gov/pubmed/16234132
http://www.ncbi.nlm.nih.gov/pubmed/22554869
http://www.ncbi.nlm.nih.gov/pubmed/20730418
http://www.ncbi.nlm.nih.gov/pubmed/16483730
DOx & Amphetamines
http://www.ncbi.nlm.nih.gov/pubmed/1208759
Ketamine & Caffeine
http://onlinelibrary.wiley.com/doi/10.1111/j.1742-7843.2009.00382.x/full
Ketamine & Alcohol
http://onlinelibrary.wiley.com/doi/10.1002/jemt.22045/abstract
Ketamine & GHB/GBL
http://www.ncbi.nlm.nih.gov/pubmed/16483730
Ketamine & Opioids
http://www.ncbi.nlm.nih.gov/pubmed/21224020
Tramadol & SSRIs
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2714818/
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2750095/
MXE & DXM
{kind=link}
http://www.sciencedirect.com/science/article/pii/S0014488607002543
MXE & Amphetamines
http://www.ncbi.nlm.nih.gov/pubmed/25060403
DXM & PCP
http://www.sciencedirect.com/science/article/pii/S0014488607002543
PCP & SSRIs
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1224745/
Amphetamines & Benzodiazepines
http://www.ncbi.nlm.nih.gov/pubmed/17320309
MDMA & Caffeine
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3492978/
http://link.springer.com/article/10.1007/s00213-010-1864-1
http://www.sciencedirect.com/science/article/pii/S0028390805003114
http://www.ncbi.nlm.nih.gov/pubmed/24211539
MDMA & Alcohol
http://www.ncbi.nlm.nih.gov/pubmed/21040238
http://www.ncbi.nlm.nih.gov/pubmed/21756931
Cocaine & SSRIs
http://www.ncbi.nlm.nih.gov/pubmed/23761390
http://www.ncbi.nlm.nih.gov/pubmed/20195220
Caffeine & Alcohol
http://www.ncbi.nlm.nih.gov/pubmed/20001110
Caffeine & Tramadol
http://www.ncbi.nlm.nih.gov/pubmed/20837047
Caffeine & SSRIs
Alcohol & GHB/GBL
http://www.ncbi.nlm.nih.gov/pubmed/15274975
Alcohol & SSRIs
http://www.ncbi.nlm.nih.gov/pubmed/15739105
GHB/GBL & Opioids
http://www.ncbi.nlm.nih.gov/pubmed/7782758
GHB/GBL & Tramadol
http://www.ncbi.nlm.nih.gov/pubmed/7782758
GHB/GBL & Benzodiazepines
http://www.ncbi.nlm.nih.gov/pubmed/16483730
GHB/GBL & MAOIs
No study, but MAO B inhibitors should enhance the effects, no interaction with MAO A.
Opioids & Benzodiazepines
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3454351/
Opioids & MAOIs
http://www.ncbi.nlm.nih.gov/pubmed/17157368 (?)
http://www.ncbi.nlm.nih.gov/pubmed/2891392
http://www.if-pan.krakow.pl/pjp/pdf/2013/3_593.pdf
Opioids & SSRIs
http://www.ncbi.nlm.nih.gov/pubmed/23391344
http://www.ncbi.nlm.nih.gov/pubmed/20513454
http://www.ncbi.nlm.nih.gov/pubmed/16005413
http://www.ncbi.nlm.nih.gov/pubmed/18676387
http://www.ncbi.nlm.nih.gov/pubmed/17381671
Tramadol & Benzodiazepines
http://www.ncbi.nlm.nih.gov/pubmed/12842359
Tramadol & MAOIs
http://www.ncbi.nlm.nih.gov/pubmed/16051647
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2750095/
Benzodiazepines & SSRIs
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2446479/
http://www.ncbi.nlm.nih.gov/pubmed/9435993